


Systemic monotherapy with rituximab is a well-known treatment approach for primary cutaneous follicle centre lymphoma and primary cutaneous marginal zone lymphoma. Both have excellent prognosis despite high relapse rates. To investigate the long-term effectiveness and clinical outcome of intravenous rituximab at a dose of 375 mg/m2 once weekly, data for 26 patients (17 primary cutaneous follicle centre lymphoma and 9 primary cutaneous marginal zone lymphoma) were analysed retrospectively. Complete remissions occurred in 20 (77%) and partial remissions in 6 patients (23%), demonstrating an overall response rate of 100%. The relapse rate was 52.9% in primary cutaneous follicle centre lymphoma and 88.9% in primary cutaneous marginal zone lymphoma. Ongoing complete remissions after therapy with rituximab were observed in 9 patients (34.6%) with a median progression-free survival of 161 months (13.4 years). These results confirm that intravenous rituximab is an effective and well-tolerated treatment with durable responses in a relevant percentage of patients at a median follow-up of 148 months (12.3 years).
Key words: primary cutaneous B-cell lymphoma; intravenous rituximab therapy; primary cutaneous marginal zone lymphoma; primary cutaneous follicle centre lymphoma; follow-up.
Accepted Jan 19, 2021; Epub ahead of print Jan 21, 2021
Acta Derm Venereol 2021; 101: adv00383.
doi: 10.2340/00015555-3746
Corr: Julia Valencak, Department of Dermatology, Medical University of Vienna, Waehringer Guertel 18-20, AT-1090 Vienna, Austria. E-mail: julia.valencak@meduniwien.ac.at
Primary cutaneous follicle centre lymphoma and primary cutaneous marginal zone lymphoma are the second most common primary cutaneous B-cell lymphomas, with high relapse rates, requiring several therapies in the course of disease. Although surgical excision or radiotherapy are recommended first-line treatments, a high proportion of patients present with multifocal disease or extended lesions. In recent decades, intravenous rituximab has been used successfully in primary cutaneous B-cell lymphomas. This study shows that intravenous rituximab is an effective and safe treatment for primary cutaneous follicle centre lymphoma and primary cutaneous marginal zone lymphoma in long-term follow-up.
The choice of therapy for primary cutaneous B cell lymphomas (PCBCL) is a challenge as this heterogeneous group of diseases is rare. They account for only 20–25% of all primary cutaneous lymphomas (PCL) (1, 2). Among PCBCL, primary cutaneous follicle centre lymphoma (PCFCL) and primary cutaneous marginal zone lymphoma (PCMZL) are the most frequent subtypes (1, 2). PCFCL and PCMZL cover more than two-thirds of PCBCL and show an excellent 5-year survival rate of 95–99% (2). Although PCFCL and PCMZL are characterized by a good prognosis, the incidence of relapses is high, varying between 25% and 68% and impairing quality of life of affected patients (2, 3).
Due to a lack of randomized controlled trials, treatment recommendations for PCBCL are based largely on small retrospective studies and institutional experience. With skin lesions preferentially occurring on the trunk (48.9%) and face (26.4%) (4), the appropriate treatment has to be carefully considered. Apart from radiotherapy and surgical excision, therapeutic options include systemic corticosteroids, interferon alpha, systemic rituximab and chemotherapy (5, 6). Rituximab (R) is a chimeric human-mouse monoclonal antibody that targets the CD20 antigen expressed both on normal and neoplastic B-cells. For the last 20 years, its effectiveness has been repeatedly confirmed in patients with B-cell non-Hodgkin lymphomas (5, 6). In patients with extensive lesions on the face and scalp, intravenous R might constitute a sensible first-line approach to avoid permanent alopecia, scarring and other irreversible cutaneous side-effects (7, 8). Several case reports and small retrospective cohort analyses have provided evidence for intravenous R as an effective treatment option in CD20-positive PCBCL (9–17). Nevertheless, no consistent data on optimal dosing intervals, number of treatment cycles and long-term treatment duration can be extrapolated from these series. So far, the median follow-up time of published reports ranges between 1 and 3 years, and sample sizes are limited to a maximum of 16 patients (9, 11–16). Currently, there is no clear evidence that maintenance treatment is able to consolidate remissions, and some reports even suggest that it should not be recommended (9). We thus performed a retrospective analysis of 26 consecutive patients with PCFCL and PCMZL treated with intravenous R, with a follow-up period of up to 12 years.
A retrospective evaluation of all consecutive patients with PCFCL and PCMZL treated at the Department of Dermatology, Medical University of Vienna, Austria, between 2003 and 2020 identified 26 patients (8 female, 18 male) undergoing monotherapy with systemic R. Patient data are shown in Table I. All data were retrospectively analysed at our institution at the department of Dermatology, Medical University of Vienna after study approval by the local ethics committee (1699/2015). Biopsy samples were consistent with the diagnosis of PCFCL and PCMZL according to the World Health Organization/European Organisation for Research and Treatment of Cancer (WHO/EORTC) classification (1). Tumour-Node-Metastasis (TNM)-stage was defined according to the TNM classification system for PCL proposed by the International Society for Cutaneous Lymphomas (ISCL) and the Cutaneous Lymphoma Task Force of the EORTC (18). None of the included patients had nodal or visceral involvement. One patient (patient number 10, Table I) had an epidural mass. In this patient, the cutaneous tumour of the PCFCL had spread directly from the head to the adjacent bone of the occipital skull.
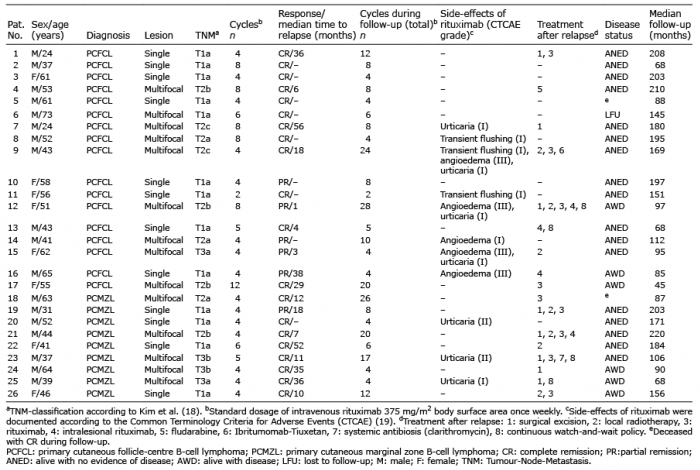
Table I. Characteristics of patients and treatment response of systemic single therapy with rituximab in 26 patients with cutaneous B-cell lymphoma (CBCL)
All patients received intravenous therapy with a standard dose of 375 mg/m2 R once weekly for 4 consecutive weeks. In 12 patients with single lesions, intravenous R was chosen due to a large lesion size (2/12), lesions located on the face or scalp and risk of disfigurement due to local treatment (i.e. surgery or radiotherapy) (8/12), or relapsed disease (2/12). Laboratory monitoring was performed before each therapy cycle. Cutaneous involvement was evaluated weekly before therapy. In patients showing complete remission (CR) of cutaneous lesions after 4 cycles, therapy was discontinued. In patients developing only partial remission (PR), i.e. size reduction in case of solitary lesions or reduction of number of lesions in multifocal disease of at least 50%, 2–4 further infusions were administered. Follow-up visits after the last treatment cycle were performed at 3–6 monthly intervals. Side-effects of rituximab were documented according to the Common Terminology Criteria for Adverse Events (CTCAE) (19).
Evaluated parameters were progression-free survival (PFS), therapeutic response in relation to the clinical presentation (single, multifocal), recurrence rates, time to relapse (TTR), number of cycles with regard to relapses as well as side-effects of systemic R in the long-term follow-up. Descriptive statistics, Pearsons χ2 test, and Kaplan–Meier curves were performed with IBM® SPSS® Statistics (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp.).
There were 18 male and 8 female patients (male:female ratio 2.25) with a median age of 51 years (range 24–73 years). Seventeen patients were classified as PCFCL and 9 as PCMZL.
Twelve patients (8 PCFCL, 4 PCMZL; 46%) had a single lesion, predominately located on the head, whereas 14 patients presented with multifocal disease (9 PCFCL, 5 PCMZL; 54%). Patient characteristics, response rates, and relapses and the specific side-effects following R are summarized in Table I.
Fourteen patients (54%) received R at first relapse after pre-treatment (Table I), 12 patients (46%) were treated with R as first-line therapy. The majority of patients (62%; 18/26) received a standard induction of 4-weekly intravenous doses of R, 8 patients received more than 4 cycles.
Twenty patients (77%) achieved CR and 6 patients (23%) had PR, resulting in an overall response rate (ORR) of 100%. Patients with PCFCL had a CR in 71%, and in PCMZL CR rate was 89% (p = 0.31). Eleven patients (42%; 6 with PCFCL and 5 with PCMZL) showed CR after the standard therapy of 4 R infusions. Independent of the number of administered cycles, a relapse was observed in 52.9% of PCFCL and 88.9% of PCMZL (relapse rate 65%; χ2(1)=3.36; p = 0.067) with a median TTR of 18.0 months (range 1–56 months). Ongoing CR after induction therapy with intravenous R was observed in 9 patients (35%) with a median PFS of 161 months (range 88–203 months). Fig. 1 shows the Kaplan–Meier curve for PFS for both entities. The median follow-up of our cohort was 148 months (range 45–220 months).
Fig. 1. Kaplan–Meier curve for progression-free survival (in months) in patients with primary cutaneous follicle-centre lymphoma (PCFCL) and primary cutaneous marginal zone lymphoma (PCMZL).
Regarding clinical presentation, 9/12 patients with a single lesion and 11/14 with multifocal disease achieved CR after induction therapy. During follow-up, 11 patients with multifocal disease and 6 with a single lesion relapsed (χ2(1)=2.33; p = 0.127).
Relapses were treated with single-agent intravenous R in 6/9 patients with PCFCL (median 16 cycles; range 8–28) and in 5/8 patients with PCMZL (median 17 cycles; range 8–26). Thirteen patients (50%) had more than one relapse (median 2.0; range 0–8). Further therapeutic regimens are summarized in Table I. The disease status at the time of evaluation, highlighted in Table I, shows that 17/26 patients (65.4%) were alive with no evidence of disease (ANED), 6/26 (23.1%) were alive with disease (AWD), and one was lost to follow-up after 30 months (patient number 8, PCFCL, multifocal disease, CR after 6 cycles). Two patients (8%) died during follow-up. In both cases, death was not disease-related.
In general, intravenous R was well tolerated and no life-threatening adverse events were observed (see Table I). In total, 42.3% of patients (11/26) experienced treatment related side-effects, most commonly urticaria grade I/II (26.9%), angioedema grade III (19.2%), or flush grade I (11.5%), which were easily manageable and none of the patients had to discontinue therapy.
In recent years, successful application of systemic R in patients with PCBCL has been published repeatedly (9–17), some reports have included a rather small sample size and a limited follow-up duration of only 3 years (9, 16, 17). However, no randomized controlled trials are available and treatment recommendations are therefore based on retrospective studies (5).
As PCFCL and PCMZL present with multifocal disease in a high percentage of cases and a high risk of local recurrence after treatment (2, 20), there is a need for an effective treatment with long remission rates and manageable side-effects.
The current study retrospectively analysed a cohort of 26 consecutive patients with PCFCL and PCMZL treated with systemic R. The main focus was to determine the long-term results of these patients, with an emphasis on PFS, recurrence rates and number of treatment cycles needed for prolonged recurrence-free intervals. In the current cohort, 18/26 patients were treated with the standard induction therapy of 4 weekly R infusions. With a median follow-up duration of more than 12 years, CR was achieved in 77% of patients and PR in 23%. None of the patients had stable or progressive disease during R treatment. One review found a CR rate of 77% and a duration of response ranging from 6 to 57 months in 44 patients with PCBCL treated with systemic R (17). This is in line with the data from the current study, which documented an ORR of 100% with 77% CR rate. In the current study population, 89% of patients with PCMZL and 71% of patients with PCFCL achieved CR.
According to the literature, recurrences after systemic treatment with intravenous R are found in approximately 20–50% of patients (10). This fact was also observed in our patient cohort, as 65% experienced a relapse after induction therapy. However, relapses were more detected frequently in PCMZL compared with PCFCL (88.9 vs 52.9%), an observation that cannot readily be explained by the molecular pathological concept of both entities. One explanation might be that PCMZL, which possibly arises from a similar pathogenetic background to that of other extranodal marginal zone lymphomas, develops in a distinct inflammatory environment that seems to be a Th2-type cytokine environment, also known to control immunity against extracellular parasites (21). In the past 15 years, several infectious agents have been identified as truly causing marginal zone lymphoma, but data on bacterial causes for non-gastric marginal zone lymphomas are rare. No significant associations between infectious agents and PCMZL have been demonstrated to date, but these are still under discussion, and unknown infectious triggers could represent the reason for the frequent recurrences in patients with PCMZL (22). Another explanation as to why systemic R might fail to achieve long-lasting progression-free intervals in PCMZL could be due to the upregulation of anti-apoptotic molecules. Wobser et al. (23) showed an upregulation of bcl-2 in relapsing PCBCL, which raises the hypothesis that modification of apoptosis-regulating proteins might be important for the efficacy of rituximab therapy. The current study further observed that patients with single lesions (CR in 75%) achieved similar response rates after induction therapy compared with patients with multifocal disease (CR in 79%). However, during follow-up initial multifocal disease was associated with a higher relapse rate of 79% and a less durable median TTR of 12 months (not significant). The fact that multifocal disease is associated with short-lived remissions has also been confirmed in previous studies in both PCFCL and PCMZL, respectively (9, 24, 25). The results of the current study patient cohort indicate that re-treatment with R after recurrence seems to be beneficial, as observed previously (16). Gellrich et al. (12) proposed that prolonged R treatment with 8 cycles might obtain better response rates than standard induction therapy with 4 cycles. In addition, further studies (16, 24) have suggested that maintenance therapy improves response and TTR. In systemic follicular lymphoma, R maintenance therapy has a beneficial effect of extending relapse-free intervals despite the association of a higher number of viral infections (26, 27). In fact, all patients in the current study were also re-treated upon relapse rather than undergoing maintenance, and the results indicate that response and time to recurrence do not necessarily need a prolonged course of R treatment, since combination therapy with radiotherapy after 4 cycles and/or a re-induction therapy using R after a multifocal relapse show excellent results with a reduced risk of side-effects.
Apart from the high clinical efficacy, R was generally well tolerated apart from the above-mentioned side-effects, which were grade I–III.
Table II shows a detailed literature review of the various therapies used in PCFZL and PCMZL with the respective TTR and response rates. A direct comparison of local treatments, such as radiotherapy and/or surgical excision with intravenous R has not been performed so far, although both are recommended first-line therapies in PCBCL (28). One study demonstrated a CR of 100% after local radiotherapy, but a relapse rate of 45% after 5 years, with a median time to recurrence of 10 months (29). Another study with 126 patients demonstrated relapses in 60% of PCMZL and 29% of PCFCL at a median of 12–16 months (30). In comparison with both studies, the current patient cohort had a prolonged relapse-free interval with a median TTR of 18.0 months. Taken together, most response rates show only minor differences and confirm the benign clinical course of both lymphomas.
Table II. Overview of the systemic rituximab therapies used in primary cutaneous follicle-centre B-cell lymphoma and primary cutaneous marginal zone B-cell lymphoma (selected studies with at least 5 patients and the respective follow-up results)
However, long-term cutaneous side-effects of radiotherapy include alopecia, chronic dermatitis, hyperpigmentation, and skin atrophy, as well as secondary skin cancers, and surgical treatment has a possible risk of scarring. Thus, intravenous R appears to be a reasonable and safe treatment for multifocal lesions, as well as for single lesions on the face and scalp.
In conclusion, the results of this study confirm that systemic monotherapy with 4 cycles of R appears to be a safe treatment option in PCBCL both for multifocal or recurrent disease or patients with single lesions in distinct anatomical sites where local treatment is less favourable. While none of the patients in this study were subjected to maintenance therapy, re-treatment after recurrence or a combination of R plus local therapy in patients with partial response seem to achieve excellent long-term results with no pronounced risk of side-effects due to the suppression of CD20-positive B-cells in the peripheral blood.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize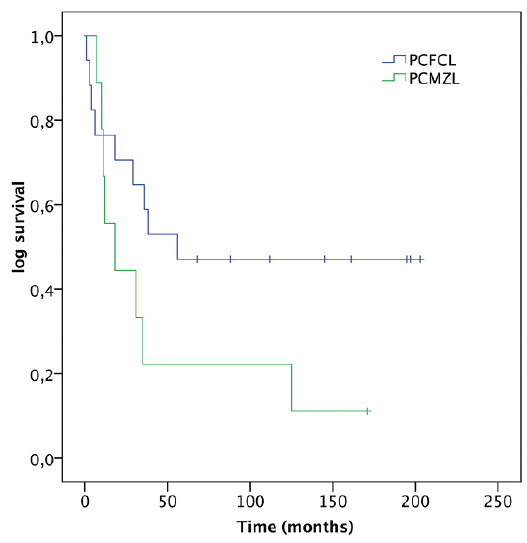 Click to show fullsize
Click to show fullsize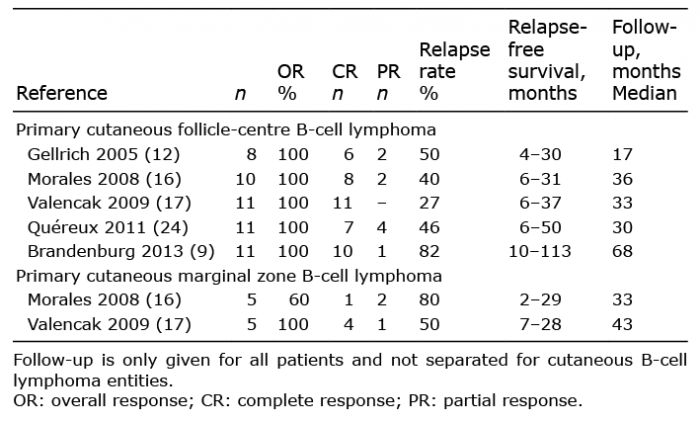 Click to show fullsize
Click to show fullsize